Before and After 2024: The Zirconia Renaissance – Unlocking the Aesthetic Potential with Strength

In the ever-evolving world of metal-free aesthetic dentistry, material selection remains one of the most powerful—yet often under-examined—decisions we make as clinicians and ceramists. Since the inception of my inaugural business in 2008, Smile by Yugo, I’ve witnessed—and contributed to—a profound transformation in the materials we rely on to craft beauty and function alike.
Over the years, we’ve transitioned from traditional feldspathic and refractory layering veneer techniques to pressed glass ceramics (e.g., Empress, Ivoclar Vivadent), exploring the potential of staining techniques in monolithic structures, then upgraded to lithium disilicate (e.g., e.max, Ivoclar Vivadent), and now, increasingly, toward the modern versatility of zirconia. That said, without ongoing engagement in continuing education, hands-on experimentation, and cross-disciplinary collaboration, it’s easy to default to familiar or outdated techniques—often at the expense of what newer materials can offer.
But dentistry, empowered by modern science and technology, rewards those who adapt. Every case I encounter presents a distinct set of clinical and aesthetic variables: preparation design, amount of reduction or final restoration thickness, optical properties of the underlying abutment, and the intended final shade—all of which must inform our material choice. Today’s zirconia offers far more than strength alone. With advancements in its translucency, gradient shading, and multi-layered formulations, zirconia has emerged not just as an alternative—but as a leading contender for the most aesthetic and durable solution in our current arsenal.
In this article, I explore the evolution of our material landscape through a case that reflects just how far zirconia has come—using e.max ZirCAD Prime (Ivoclar Vivadent)—and how understanding its full potential can redefine not only functional success, but also patient perception and aesthetic excellence.
Pre-op Condition: Listening beyond instructions


Unlike most cases where I have the privilege of being involved from the very beginning—helping to shape the treatment plan from an aesthetic standpoint—this case came with pre-set limitations. I was informed that treatment would be confined to the upper and lower six anterior teeth, totalling twelve units. While this framework gave me a starting point, it didn’t limit my priority: to understand what the patient truly wanted to achieve.
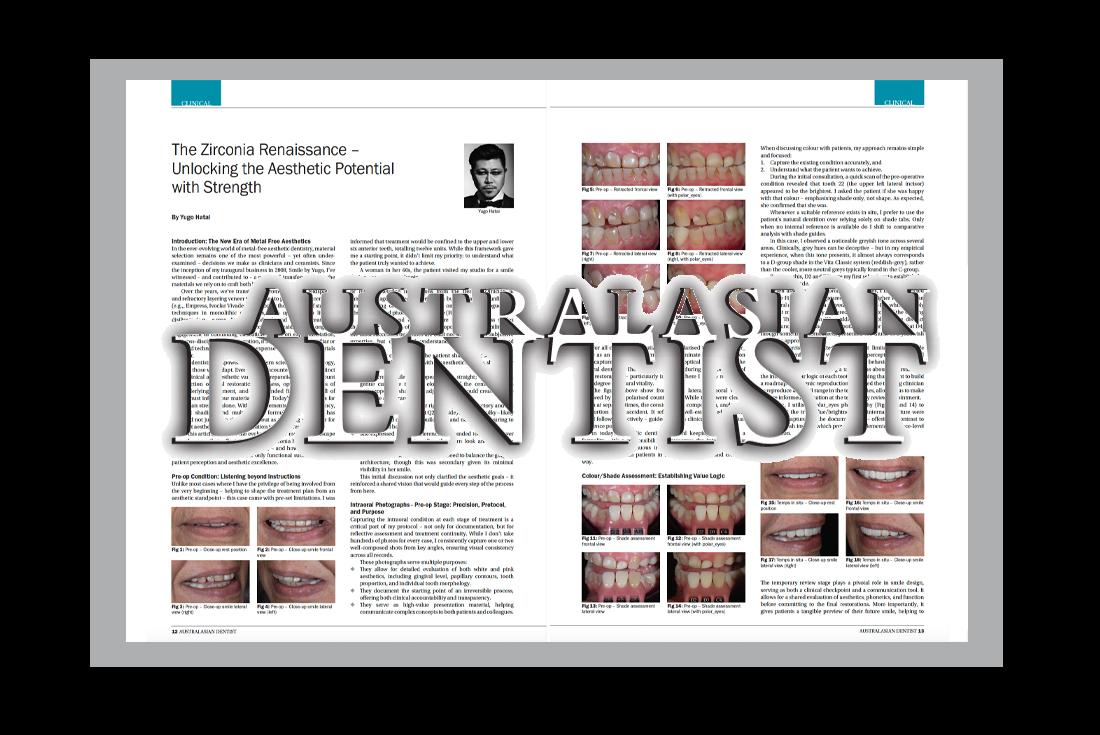
A woman in her 60s, the patient visited my studio for a smile design consultation, hoping to improve the appearance of her aesthetic zone. I deliberately chose not to study the case beforehand or rely on detailed instructions from the treating clinician at this early stage. Instead, I focused on building a fresh, unfiltered understanding of her goals—based on personal dialogue, live observation, and photographic capture (Figs 1-4).
As clinicians and ceramists, we’re trained to assess smiles through our own lens of symmetry, proportion, and feasibility. But the most successful outcomes are built not solely on our subjective expertise, but on mutual understanding between patient and practitioner.
During our consultation, the patient shared her concerns and aspirations, which, combined with my aesthetic insights, shaped our direction:
- The current smile line appeared too straight; introducing a gentle curvature through elongation of the central incisors and supportive shaping of adjacent teeth would create a more feminine appearance.
- The labial profile of Q1 (her right side) was satisfactory and did not require retroclining, but Q2 (left side) appeared bulky—likely due to the old composite build-up—and needed contouring to restore facial balance.
- She expressed a clear preference for rounded tooth forms over square ones, aiming to soften the worn look and reclaim a youthful vibrancy.
- The treating clinician also noted the need to balance the gingival architecture, though this was secondary given its minimal visibility in her smile.
This initial discussion not only clarified the aesthetic goals—it reinforced a shared vision that would guide every step of the process from here.
Intraoral Photographs – Pre-op Stage: Precision, Protocol, and Purpose



Capturing the intraoral condition at each stage of treatment is a critical part of my protocol—not only for documentation, but for reflective assessment and treatment continuity. While I don’t take hundreds of photos for every case, I consistently capture one or two well-composed shots from key angles, ensuring visual consistency across all records.
These photographs serve multiple purposes:
- They allow for detailed evaluation of both white and pink aesthetics, including gingival level, papillary contours, tooth proportion, and individual tooth morphology.
- They document the starting point of an irreversible process, offering both clinical accountability and transparency.
- They serve as high-value presentation material, helping communicate complex concepts to both patients and colleagues.
For all cases I treat, I utilise cross-polarised filters (e.g., polar_eyes) as additional information to eliminate surface reflection and capture the internal structure and optical behaviour of the natural dentition. This data is invaluable during the fabrication of final restorations—particularly in cases where I aim to replicate a high degree of natural vitality.
The figures above show frontal and lateral intraoral views, followed by their polarised counterparts. While these were clearly taken at separate times, the consistency in composition, angle, and proportion is no accident. It reflects a well-established protocol that I follow instinctively—guided by both clinical logic and visual reference points.
In today’s aesthetic dentistry, record keeping is not just a formality—it’s a responsibility. It preserves the integrity of our work, supports continuous improvement, and allows for open communication with patients in a visually engaging and credible way.
Colour/Shade Assessment: Establishing Value Logic


When discussing colour with patients, my approach remains simple and focused:
- Capture the existing condition accurately, and
- Understand what the patient wants to achieve.
During the initial consultation, a quick scan of the pre-operative condition revealed that tooth 22 (the upper left lateral incisor) appeared to be the brightest. I asked the patient if she was happy with that colour—emphasising shade only, not shape. As expected, she confirmed that she was.
Whenever a suitable reference exists in situ, I prefer to use the patient’s natural dentition over relying solely on shade tabs. Only when no internal reference is available do I shift to comparative analysis with shade guides.
In this case, I observed a noticeable greyish tone across several areas. Clinically, grey hues can be deceptive—but in my empirical experience, when this tone presents, it almost always corresponds to a D-group shade in the Vita Classic system (reddish-grey), rather than the cooler, more neutral greys typically found in the C-group.
Based on this, D2 and D3 were my first selections to establish the primary base shade.
When assessing the chroma of the canines, I initially selected A3.5 (see Fig. 11), but it appeared too bright—higher in value than the natural dentition. I then moved to C4 (Figs 12–14), which is rarely used, but more accurately captured the deeper tone of the existing canines. That said, even C4 couldn’t quite replicate the distinct reddish undertone I observed in tooth 23. It’s worth noting that D4, though sometimes considered, presented too much of a yellowish cast to be appropriate here.
This exercise highlighted the inherent limitations of shade guides and reinforced the value of trained perception and clinical judgement when interpreting natural colour behaviour.
This wasn’t about matching a tab—it was about understanding the internal colour logic of each tooth and using that insight to build a roadmap for ceramic reproduction. I advised the treating clinician to reproduce a D2/D3 range in the temporaries, allowing us to make a more informed evaluation at the temporary review appointment.
Again, I utilised polar_eyes photography (Figs 12 and 14) to ensure that the true value/brightness and internal structure were accurately captured in the documentation—offering a contrast to standard flash images, which provide complementary surface-level information.
Temp Review:


The temporary review stage plays a pivotal role in smile design, serving as both a clinical checkpoint and a communication tool. It allows for a shared evaluation of aesthetics, phonetics, and function before committing to the final restorations. More importantly, it gives patients a tangible preview of their future smile, helping to refine expectations and build confidence in the treatment direction.
In this case, the patient is generally satisfied with the shape of the temporaries. That said, while the labial position of the centrals has been idealised, I feel the overall smile curvature can be accentuated further—specifically by slightly increasing the length of the central incisors and shortening the canines (particularly tooth 13).
Intraoral Photographs: Temps in Situ


The intraoral photographs illustrate the current condition of the gingival architecture. A gingivectomy was performed at the time of preparation, so the tissue levels are not yet finalised—providing an opportunity to influence the final gingival contours through ceramic design.
This transitional stage gives me some control over the soft tissue response, particularly through the manipulation of emergence profiles. For instance, I aim for the gingival margin in Q1 to rebound and regenerate naturally. Conversely, in select areas, I intend to guide the tissue further coronally by applying pressure with a carefully designed emergence profile—adding subtle bulk at the margin or cervical third—to effectively increase crown length and enhance symmetry.
Colour/Shade Assessment: Temps in Situ


The patient is generally happy with the provisional restorations, which were produced in a shade close to D2. This was a deliberate choice based on our initial smile design consultation, intended to guide the final value selection for the definitive restorations.
At this stage, I want to emphasise the importance of using polar_eyes photography for value assessment. While the D2 shade may appear slightly greyer—or lower in value—in Figures 23 and 25, this is not the case in Figures 24 and 26. In my experience, polarised images provide a far more reliable reference for brightness and value, compared to conventional twin flash photography, which can mislead due to surface reflection and gloss.
During the review, I also discussed my intention to increase the depth of colour slightly toward the canines. In practical terms, I’m comfortable using a D2 base shade for teeth 12 to 22, while enhancing the chroma at the canines—transitioning to a D3 base for a more natural and harmonious gradient. It’s important to communicate these subtle aesthetic nuances with the patient at this stage. If they prefer a more uniform appearance across the arch, I’m happy to honour that choice (although such requests are rare).
Ultimately, I offer what I believe to be the most aesthetic and natural outcome from my perspective—but where disagreement arises, I set my ego aside and follow the patient’s instruction. This approach prevents misalignment or potential remakes during the try-in or final insertion stages, ensuring a smoother and more collaborative process. Likewise, I tend to prioritise the patient’s request over clinical philosophy—unless I strongly agree with the clinician’s rationale for logical and aesthetic reasons. After all, it is the patient—not us, the dental professionals—who must live with the outcome, and they remain the final and most important judge of success.
Framework Design:

At this stage, I’d like to highlight the benefits of using e.max ZirCAD Prime—a next-generation zirconia that redefines what’s possible in restorative design. According to Ivoclar, ZirCAD Prime features a continuous gradient structure, transitioning seamlessly from high-strength dentine zirconia (≥1200 MPa) to more translucent enamel-like layers. This innovative composition enables restorations to retain maximum strength in the core while delivering exceptional aesthetics at the incisal edge—effectively overcoming the harsh opacity seen in earlier zirconia generations.
This allows us to preserve the zirconia structure right through to the incisal edge without compromising visual quality. While some clinicians advocate for full-contour monolithic restorations using only staining techniques, I support that approach only to an extent. In the aesthetic zone, I remain a strong advocate for minimal but strategic layering ceramics, particularly in the incisal third, to achieve natural translucency, depth, and lifelike surface texture.
Figures 27 and 28 show the framework design developed in close collaboration with Mr. Jay Woo (Mowbray Dental)—my former employee positioned as CAD/CAM manager from the Smile by Yugo era, who continues to manage the digital workflow and CAD/CAM production in my current practice at Smile Virtuoso today. Together, we approached this case with careful attention to material properties and anatomical fidelity.
Generally speaking, the more zirconia structure we can preserve, the greater the inherent strength of the final restoration. This enables clinicians to adopt more conservative preparation protocols, supporting the minimally invasive philosophy at the core of modern aesthetic dentistry.
However, this conservative approach results in naturally thinner restorations. Therefore, when anatomical cut-back is indicated, extra precision is required to recreate mamelon structure and incisal character, ensuring we maintain both functional strength and aesthetic integrity.
While e.max ZirCAD Prime sits at the high end of the market in terms of cost, I believe its performance potential fully justifies the investment. In this case, although some elements of the protocol remain experimental, I was pleased with the outcome. It not only strengthened our internal design strategy but also reaffirmed my belief in using only the very best materials available for each case I treat. This material certainly met—and continues to meet—those expectations.
Virtual Try-in of the Final Restorations: The Aesthetic Articulator


One of the defining tools in my workflow is the Aesthetic Articulator—a patented invention of mine, granted in 2013—developed to elevate the precision and predictability of smile design prior to case dispatch. Over a decade later, in 2025, I remain convinced that no current 3D CAD/CAM-based technology has surpassed this method in terms of visual accuracy and control. This is why I continue to use this technique in my workflow today. The Aesthetic Articulator allows for highly detailed visualisation of the final restorations—well beyond what conventional laboratory protocols typically provide. By simulating both the static and dynamic aspects of the smile, it enables me to refine form, proportion, and spatial balance with clinical precision and artistic integrity—ensuring that each restoration is not only technically correct but facially and aesthetically optimised.
Figure 29 shows the modified framework fabricated in e.max ZirCAD Prime (Ivoclar Vivadent). The material’s high strength and improved translucency allow me to extend the zirconia substructure to the full incisal edge and final crown length—maximising structural integrity with minimal reliance on layering ceramic as discussed earlier. However, I still balance both incisal length and gingival height with strategic ceramic layering. This is guided not only by aesthetic intuition but by reliable, calibrated reference points—as marked by the numerical horizontal guides.
Figures 30–32 present the virtual try-in of the final restorations on the Aesthetic Articulator. While the final colour accuracy is best verified intraorally, the morphology, proportion, and spatial dynamics can be judged with high confidence. Personally, I was satisfied with the outcome, and with final checks completed, the case was cleared for dispatch to the dental practice for insertion.
Post-operative Outcome:


Figures 33–36 show the post-operative condition, which was evidently successful—and closely aligned with the virtual outcome established through my patented Aesthetic Articulator. The case was well received by both the clinician and the patient, as is consistently the case with this protocol. The patient kindly left a heartfelt Google Review, further validating my approach and reinforcing its effectiveness to both the general public and referred patients.
She shared that it had taken 16 years to finally achieve the smile she had always envisioned. Her words were filled with gratitude and emotion—now able to smile with genuine confidence for the first time in decades.
It’s also worth noting that she is in her 60s—yet the transformation reached far beyond her dentition. The smile, paired with the confidence behind it, gave her a renewed sense of presence. She looked absolutely radiant—not only because of the aesthetic result, but because of the self-assurance it brought forward.
As I often say, my job is to help people fall in love with their smile—and in this case, I can confidently say: mission accomplished.
Intraoral Photographs – Post-op:



Figures 37–42 present detailed intraoral photographs of the final outcome—a reflection of my continued commitment to full transparency in case presentation. I have nothing to hide, and as always, I believe that sharing clear, unedited images is essential to uphold the integrity of our craft—especially in a time when modern dentistry is increasingly disrupted by social media and digital manipulation. Authenticity matters, and these images speak for themselves.
I would also like to acknowledge Dr Peter Ong from Top Care Dental Boutique in Menai, NSW, Australia, for his outstanding clinical work. His precision and consistency—from the initial treatment planning to the final delivery—played a crucial role in the success of this case. It is always a privilege to collaborate with clinicians who uphold the same standard of excellence and patient-focused care.